ALGORITHM FOR THE DIAGNOSIS AND TREATMENT OF SHOULDER DISORDERS FOR HEALTH CARE PROVIDERS
Approach to the Shoulder
Seven entities account for the pain experienced by an estimated 95% of patients who present with shoulder pain. Rotator cuff disease is far and away the most important accounting for about 75% overall. The list below shows these entities in descending frequency.
- Rotator cuff disease – Tendinitis, Strain, Partial Tear or Complete Tear: Diagnosed through History and MRI
- Glenohumeral Joint Arthritis: Diagnosed through physical exam and Grashey view X-Ray
- A-C joint inflammation: Diagnosed through Physical Exam
- Glenoid Labrum Superior (SLAP) Tears: Diagnosed through history and MRA
- Frozen Shoulder: Diagnosed through physical exam and Grashey view X-Ray
- Cervical Radiculitis, Trapezius and Neck Strain: Diagnosed through physical exam
- Shoulder dislocation: Diagnosed through history, X-Ray and MRI
Much Less Common
Thoracic Outlet Syndrome; Tumor: benign or malignant; Pectoral Tendon Tear; Scapular Winging
Diagnosis of Shoulder Problems
The following is an algorithm for accurate diagnosis of shoulder pain.
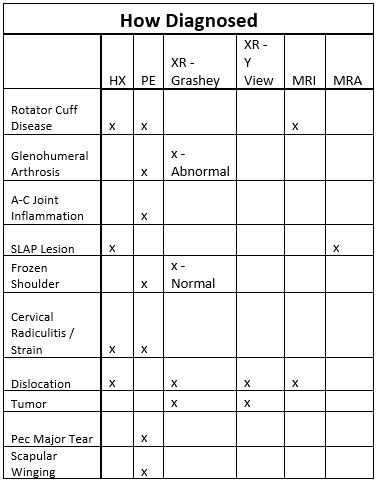
The grid shows a stepwise progression to diagnose the patient’s shoulder pain.
- Take History of trauma or overuse
- View Grashey and Y X-Ray views
- Palpate the AC joint
- Perform Hawkins Maneuver
- Test Passive supine shoulder ROM
- Direct patient to perform Wall pushup
If Clinically Indicated May Also:
- Test triceps strength
- Do Pec Major stress test
What To Look For:
- Look at the X-Ray Grashey view:
Normal joint space = No Arthritis
Decreased joint space = Arthritis - Look at the X-Ray Y view:
Normal = No Dislocation
Abnormal = Dislocation - Palpate the AC joints:
Symmetrically Tender = Normal - One side hurts more = AC Joint Inflammation
- Perform Hawkins Maneuver:
Normal = No RC Disease
Abnormal = RC disease - Examine ROM supine:
Decreased with normal Grashey = Frozen shoulder
Decreased with abnormal Grashey = Arthritis - If History of traction or impaction of affected arm may be SLAP lesion. If pain is posterior this is likelier. If no other diagnosis exists must get MRA.
- If patient has pain in neck, medial scapular and radiating down posterior arm, lateral forearm and numb fingers and an asymmetrically weak triceps on the affected side it is cervical radiculitis.
- If they have discomfort and limitation with leftward and rightward neck rotation it is cervical strain.
- If they have pain in the trapezius it is trapezius strain - But Often This is Secondary to AC Inflammation, which is diagnosed by AC palpation as above.
- If Y or Grashey view x-ray is positive for dislocation, then it is an unreduced dislocation. If a patient has a history of feeling shoulder come completely out of joint and then going back in then it is reduced shoulder dislocation. MRI can confirm dislocation.
- If x-ray is positive for lytic or blastic lesion it is tumor, which should be confirmed by MRI. All suspected tumors should be immediately referred to an orthopaedic surgeon.
- If a patient has traumatic history, usually an eccentric pec contraction as with a bench press with the bar going down, and physical exam is positive for webbing then pectoral rupture
- If posterior scapular discomfort, and on winging present when performing a wall pushup, then winging scapula.
Treatment of Shoulder Problems
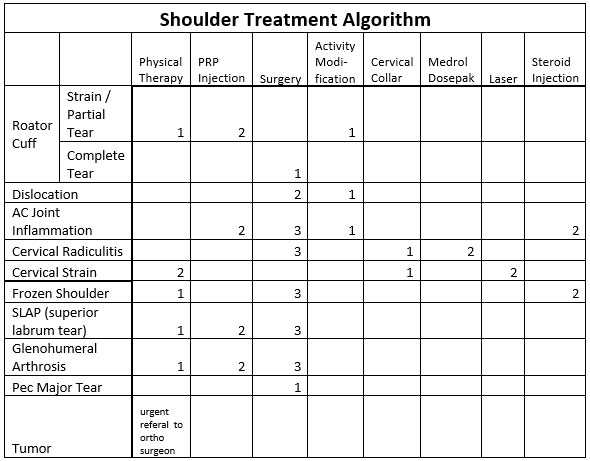
The above chart is labeled with the appropriate treatments to try first (1), second (2) or third (3) for each diagnosed problem.