Shoulder Dislocation
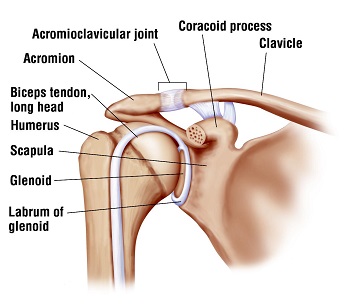
Anatomy: The glenohumeral or shoulder joint can suffer dislocation when the “ball” at the top of the humerus or arm bone is ripped out of the glenoid or “socket.” Generally the arm dislocates forward and inferiorly. The anterior inferior glenohumeral ligament is torn and usually the labrum is detached from the glenoid, the so-called “Bankart” lesion.
Injury: Usually the arm is elevated out to the side and backward resulting in the injury, although other mechanisms are possible. The arm may spontaneously “reduce” (return to the socket) or may require treatment in an emergency room to be put back in place.
Diagnosis: Diagnosis is obvious if an X-ray is taken when the shoulder is dislocated. If this does nto happen diagnosis is made by the history primarily, by the exam to some degree, and with some help from MRI.
Treatment: After the first dislocation treatment is generally non-surgical consisting primarily of protected activity for several months to allow healing of the ruptured ligament. If the dislocation recurs a second or third time surgery is often performed. I was fortunate to be trained by Dr Carter Rowe at Harvard and the Massachusetts General Hospital who was the foremost Orthopaedic Surgeon in the world in the treatment of this problem using a surgical procedure called a Bankart repair. I have used this procedure, when surgery is necessary, for over thirty years with excellent results, including in professional athletes.