ACL (Anterior Cruciate Ligament)
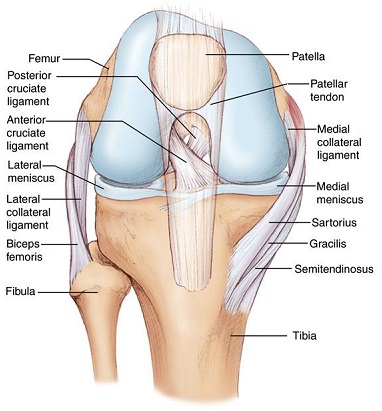
Anatomy: The Anterior Cruciate Ligament runs down the center of the knee. When it is torn the knee is unstable.
INJURY: The ACL tears by several mechanisms including twisting and a blow to the outside of the knee. There is usually immediate marked swelling. However after a few weeks pain may disappear entirely leaving the injured patient with a false sense that the knee has healed. In fact, chronically torn ACLs produce cartilage damage and arthritis and are a leading cause of premature knee replacement surgery in young people.
The ACL Textbook & My Research: As a result of pioneering work I did in the field of ACL reconstruction surgery II was asked by my peers to be editor in chief of the first and only comprehensive textbook on the ACL for Orthopaedic Surgeons, the second edition of which will be released this year.
Diagnosis: The history of a twisting injury accompanied by immediate marked swelling is suggestive of but not confirmatory of ACL tear. The Lachman test on physical exam is helpful and the KT1000 arthrometer, which is an instrumented Lachman test is the most accurate test of complete ACL tear with an accuracy rate above 95%. MRI is also useful, but in one of our publications we found a 19% MRI ACL error rate.
Treatment: Complete ACL tears should generally be repaired to preserve function and prevent arthritis. Patients well into their 50s are good candidates, sometimes older in fit active individuals. If the torn ACL is not reconstructed most patients will develop premature arthritis. I have published the largest series of hamstring ACL reconstructions in the world’s literature. In this series we had no graft failures. I use only the hamstring tendon as a graft. This is the strongest and most widely used graft and results in less kneeling pain than patellar tendon grafts. I also specialize in reconstructing the ACL in patients with previous graft failures, and have a high rate of success in doing so. Surgery is outpatient and patients are usually full returned to sports activities six months after surgery.
Joint Distraction Arthroplasty (JDA)
You will need the Adobe Reader to view and print these documents.